NIOSH Fatality Assessment and Control Evaluation (FACE) Program
|
Telecommunications Tower Maintenance Worker
Struck By Cable In Nebraska
|
| Nebraska Case Report: 02NE013 |
Report Release Date: November 18, 2002
|
SUMMARY: (top)
A 29-year-old telecommunication tower line supervisor was killed when the wire rope being used to hoist coaxial cable broke, allowing the cable and other materials to strike him. The victim was part of a five person crew that was hoisting coaxial cable up on the outside of a 1524 foot high telecommunications tower. The victim and two other workers were approximately 1100 feet up on the tower, guiding the coaxial cable to prevent it from banging into the tower side. The  victim was outside of the tower structure, standing on a “platform” which was an ice guard above an FM antenna. He was wearing a harness/lanyard and was tied off to the guard structure. One worker was a few feet above him and another a few feet below him, both inside the tower structure and tied off. The coaxial cable had a 350 pound headache ball attached to the end to prevent cable twisting. This was several feet above the victim. With approximately 75 more feet to go, the winds had started to become a factor at that height. The supervisor on the ground radioed the victim to have him tie the cable off where it was and they would start again the next morning if the wind died down. The victim told the owner they still had a few minutes before the wind was too high, and since they were about done, to go ahead and finish hoisting the cable. The owner went to the trailer that contained the winch, revved the motor and started to pull the handle to raise the cable. As he pulled back, he heard a “snapping” sound from somewhere up on the tower, looked up, and saw the cable, wire rope and headache ball falling towards the ground. He yelled to the other workers to get out of the way and ran to the corner of the adjoining support building. As the materials fell they struck the victim, knocking him off the platform. The materials continued downward until they fell across a guy wire, causing them to slide off to the east of the tower structure. This motion caused the entire tower structure to shake violently. The two workers, one above and one below the victim, immediately started down the structure. They radioed the owner that the victim was badly hurt. They attempted to check for a pulse but the victim was too far out on, and below the platform for them to reach. The owner told them to exit the tower immediately, as he was also afraid it was going to collapse. Local rescue personnel were summoned, but no one had the experience necessary to attempt a rescue at that height. A climbing team trained in rescue procedures was brought in approximately 9 hours later and the victim was removed. victim was outside of the tower structure, standing on a “platform” which was an ice guard above an FM antenna. He was wearing a harness/lanyard and was tied off to the guard structure. One worker was a few feet above him and another a few feet below him, both inside the tower structure and tied off. The coaxial cable had a 350 pound headache ball attached to the end to prevent cable twisting. This was several feet above the victim. With approximately 75 more feet to go, the winds had started to become a factor at that height. The supervisor on the ground radioed the victim to have him tie the cable off where it was and they would start again the next morning if the wind died down. The victim told the owner they still had a few minutes before the wind was too high, and since they were about done, to go ahead and finish hoisting the cable. The owner went to the trailer that contained the winch, revved the motor and started to pull the handle to raise the cable. As he pulled back, he heard a “snapping” sound from somewhere up on the tower, looked up, and saw the cable, wire rope and headache ball falling towards the ground. He yelled to the other workers to get out of the way and ran to the corner of the adjoining support building. As the materials fell they struck the victim, knocking him off the platform. The materials continued downward until they fell across a guy wire, causing them to slide off to the east of the tower structure. This motion caused the entire tower structure to shake violently. The two workers, one above and one below the victim, immediately started down the structure. They radioed the owner that the victim was badly hurt. They attempted to check for a pulse but the victim was too far out on, and below the platform for them to reach. The owner told them to exit the tower immediately, as he was also afraid it was going to collapse. Local rescue personnel were summoned, but no one had the experience necessary to attempt a rescue at that height. A climbing team trained in rescue procedures was brought in approximately 9 hours later and the victim was removed.
The Nebraska Workforce Development, Department of Labor’s Investigator concluded that to prevent future similar occurrences:
-
Employers should comply with established industry safety guidelines.
-
Employers should ensure equipment is adequate in size and strength, properly maintained and safely utilized for the job being performed.
-
Employers should ensure that adequate rescue equipment/personnel are available.
-
Employers should routinely conduct scheduled and unscheduled worksite safety inspections.
-
Employers should consider supplementing worker training on safe work practices with discussions of FACE case reports and other related training aids.
-
Tower owners should, through the use of contractual language, ensure that employers/workers adhere to OSHA-required safety measures (including Compliance Directive 2-1.29) while construction or maintenance is being performed on their towers.
PROGRAM OBJECTIVE: (top)
The goal of the Fatality Assessment and Control Evaluation (FACE) workplace investigation is to prevent work-related deaths or injuries in the future by a study of the working environment, the worker, the task the worker was performing, the tools the worker was using, and the role of management in controlling how these factors interact.
This report is generated and distributed solely for the purpose of providing current, relevant education to employers, their employees and the community on methods to prevent occupational fatalities and injuries.
INTRODUCTION: (top)
On April 22, 2002 at approximately 12:40 p.m., a 29-year-old telecommunications tower worker died after the wire rope being used to hoist coaxial cable broke, allowing it, the coaxial cable and a 350 pound headache ball, to fall and strike the victim. The Nebraska Department of Labor was notified of the fatality the same day b the Occupational Safety and Health Administration (OSHA). The Nebraska FACE Investigator met with the investigating OSHA Compliance Officer (COSHA), company officials and employees, and county and local law enforcement personnel at the incident location on April 23 & 24, 2002.
The employer is a telecommunications tower construction, testing and maintenance company. They had been in business as a registered company just over a year prior to the incident. The owner/site supervisor had previously performed this service for several years with other employers. At the time of the incident there were five employees on site. The company co-owner stated during interviews that they do have a written safety program at their headquarters, but it was not available for review at the time of this investigation. Tailgate talks were always conducted each morning and documented. Any training given to employees was done verbally and “hands-on” with documentation which was not available during this investigation. The employer has no previous history of fatalities.
INVESTIGATION: (top)
Victim: The victim was a 29-year-old male experienced in tower climbing. He had worked for another company for five years erecting high rise billboards and signs prior to joining the current employer. He had worked for the current employer for approximately two years. The day of the incident was his first day on this particular job site.
Training: The victim, along with all other employees, had previous tower experience prior to current employment. Training on rigging, personal fall protection rescue, CPR & first aid, etc. was conducted at their headquarters location. All personnel interviewed stated that they always conducted “tailgate talks” prior to performing their daily tasks. During interviews, all employees displayed adequate knowledge concerning fall protection. Note: Training records were not available for review by this investigator.
Worksite: The job site is located in a rural, isolated area approximately 18 miles south of the nearest town. Access to the site is gained by traveling 15 miles on a blacktop rural two lane highway, then the remainder on a county maintained gravel/dirt road. The transmission tower site has been there since 1967. This tower was erected in 1987 to replace one that collapsed a year earlier in an ice storm. The telecommunications tower is a 1524 foot high “guyed” structure that is maintained by on-site technicians. A contract had been awarded to a general contractor several months prior to this incident that called for the installation of 4 ½” diameter coaxial cable to establish a digital television signal. This would require hoisting the cable approximately 1200 feet up the tower. Emergency personnel services were 18 miles north of the site. They consisted of a volunteer fire department and rescue service. There is phone service available at the site.
ANALYSIS/SYNOPSIS: (top)
During the month of October, the general contractor subcontracted the project to another tower company to install the cable. This company rigged the tower prior to the first pull attempt. A block & tackle unit rated at 3 tons was installed ten feet above ground level. It was secured to the tower with a 3/8” wire rope sling and ½” shackles. An additional block & tackle unit rated at 3 tons was installed at the top of the tower in the same fashion. In between, where the tower guy wires were attached, double shackles to guide the wire rope were attached (4 total). Several attempts to hoist the cable were made, but due too bad weather, they were only able to raise it approximately 20 feet. The company left prior to the end of November. All of the equipment was left in place (wire rope, block & tackle, etc.).
The victim’s company was subcontracted to finish the job. Although they had not worked on a structure this high, they agreed to the job. Prior to the incident date, the company was performing work on a similar, but shorter, telecommunications tower approximately 225 miles west of the incident site. When that job was almost complete (April 16th), the owner and two employees left that job site to come to the incident site to survey the tower and equipment. The two employees climbed the tower and inspected the wire rope, block & tackle units and all associated shackles and wire rope slings, finding no abnormalities. Both employees stated they were given on-the-job training regarding the inspection of wire rope when they first joined the company.
The victim’s first day on site was the day of the incident. He and two other employees (workers 1 & 2) climbed the tower in preparation to starting the hoist operation. The owner and another employee (worker 3) remained on the ground to operate the hoisting equipment. The hoisting equipment consisted of 3/8” wire rope wrapped around a winch. The winch was powered by a 20 HP Kohler engine. Both were mounted on a trailer, which was tied off to a nearby power pole by a wire sling to prevent it from being drawn toward the tower.
The victim and workers 1 & 2 climbed the tower to assist in the hoist. Part of their job was to ensure that the coaxial cable did not bang against the tower while being hoisted. It is believed that all three were inside the tower guiding the coaxial cable during the initial part of the hoist.
As the hoisting began, the drum hoist engine was able to pull the cable and associated weight. The cable weight 2 ½ lbs. per foot. There was also a 350 pound “headache” ball attached to the end of the coaxial cable. This helped to lessen the twisting of the coaxial cable that occurs from being on a large reel and to stabilize it in the wind. At some point during the hoist the engine was not able to steadily pull the cable and began to sputter. The owner then “shock loaded” the engine. This consisted of revving up the engine, then engaging the pull handle. This would cause the cable to move up short distances (10-15 feet) at a time. Witnesses stated that it was a smooth motion, with no noticeable jerking of the cable.
The owner stated to assist the primary winch he knew a “capstan’s head” electrical hoist would need to be mounted to the front of a truck positioned behind the trailer. A line from this hoist would be attached to the wire rope between the main hoist and lower block and tackle unit using a “pork chop” device. This device is slipped over the main hoist line and clamps down on the wire rope. The more pressure applied, the more it clamps. As the main hoist pulled the wire rope towards it, the capstan’s head host line would “assist” by reeling in towards its hoist. When the “pork chop” device came close to the capstan’s head drum, slack would be applied and the “port chop” repositioned towards the tower for another pull. It was worker 3’s job to run this hoist. One person interviewed stated that the capstan’s hoist was being used at the time of the accident and that enough pressure was being applied that it was sliding the front of the truck slightly towards the tower.
The wind started to increase some (10-15 mph at ground level) causing the cable to be blown away from the tower. As the cable reached approximately 1125 feet high, the owner radioed the workers on the tower. He said that the wind was high enough they should “dog” (secure) the cable where it was and finish the job in the morning. The victim radioed back that they were only about 75 feet from the finish point, and that it would just take a few more minutes to finish and to continue the lift.
At this time worker 1 was above the victim, while worker 2 was below the victim. Both were inside the tower structure and tied off. None of the tower climbers wore hardhats, as the wind velocity at that height would snap the straps and blow them off. Personnel on the ground did wear hard hats. The victim had walked out on top of a metal ice guard that is used to shield an FM antenna directly below the guard. The ice shield is approximately 12 feet long by 6 feet wide. The victim hooked his lanyard to the shield and proceeded to hold the cable away from the structure.
The owner went back to stand beside the hoist trailer. He revved up the engine and reached for the pull handle. As he started to pull it back he heard a snapping sound coming from the tower area. He saw the wire rope go slack, looked up and saw debris falling downwards. He yelled for everyone to run and he ran to the corner of an adjoining support building.
Worker 1 had his head stuck outside the tower structure, pulled it back inside and turned towards the cable as he saw the wire, cable and headache ball drop by his position. He stated the coaxial cable, wire rope and headache ball “shot” towards the victim. Some portion of these items struck the victim, knocking him from the ice guard. His lanyard deployed, causing him to hang seven feet below the guard’s outside edge. The debris continued falling downward and hit at least one guy wire, causing the debris to slide along the entire length of the east guy wire. This motion caused the entire tower to shake violently. Witnesses stated that it made a high pitched shrieking sound.
Workers 1 & 2 felt the tower shake and looked down, seeing what they thought was a guy wire that had frayed. Knowing there was a possibility of a total tower collapse if this guy wire broke, they started to exit the tower as fast as they could. The owner radioed them to see if everyone was okay. They radioed back that the victim had been hit, and that it “didn’t look very good”. The owner asked them if they could reach the victim to check his condition. Both workers attempted to get to the victim. He was hanging approximately 4 ½ feet away from the tower’s edge. They were unable to get close enough to check for a pulse. They stated that visually they knew he was hurt badly and continued on down the tower.
A witness ran to call emergency personnel. It took approximately 20 minutes for them to arrive. No one was trained in tower rescue. Numerous calls were made trying to find someone that could rescue the victim. An airborne attempt was considered using a military helicopter, but abandoned due to high winds. Many different emergency response personnel/agencies arrived on scene. After collaboration the local emergency entities decided to declare the rescue beyond the local scope and the State’s Emergency management office was called. Six fire and rescue personnel from the State’s capitol fire department’s Urban Search & Rescue Team were brought to the nearest airport by a National Guard plane then transported to the accident site, arriving at approximately 5 p.m. The victim’s condition was being monitored using a hunting rifle spotting scope. At some point the on-scene commander determined that the rescue mission was now a retrieval mission. Two additional climbers from the local area were located that had some tower experience and they joined the retrieval team at the site. After determining the safest method of recovery, six members of the team proceeded to climb the tower. It took one hour and forty minutes to reach the victim. At 9:10 p.m. they started the descent. Due to the length of their retrieval ropes they could descend approximately 300 feet every 45 minutes, then had to stop and reposition their equipment. When they were approximately 90 feet from ground level they were able to place the victim in the basket of a boom truck that was on site. The victim was finally lowered to the ground at 12:05 a.m.
On May 8, 2002 the OSHA compliance officer revisited the site, accompanied by a certified rigging specialist. The specialist reviewed all the material associated with this incident and determined the following:
-
The company had used inadequate strength wire-hoisting rope that had become nicked and stretched through misuse.
-
The drum hoist being used was inadequate for the job, causing the employees to “shock load” the lifting wire.
-
The upper “snatch block” pulley atop the tower was damaged.
-
The employees were using improperly fabricated slings and wire rope eye connections.
-
There was no accident-prevention plan.
-
There was no documentation of equipment inspection to show faulty equipment.
CAUSE OF DEATH: (top)
According to the death certificate the cause of death was: Skull Fracture.
RECOMMENDATIONS/DISCUSSION: (top)
Recommendation #1: Employers should comply with established industry safety guidelines.
Discussion: During the course of investigation it was discovered that the wire rope being used to hoist the coaxial cable was inadequate for this particular task. It was rated to lift 2,800 pounds but was being used to lift 4,372 pounds. This wire was also nicked and stretched through misuse. The snatch block at the top of the tower was also damaged which may have contributed to the damage tot he wire rope. The slings being used to hoist the coaxial cable were improperly fabricated as were the “wire rope eye” connections.
The drum hoist being used to lift the wire rope attached to the coaxial cable was inadequate for the job. Because of this the lifting wire had to be “shock loaded”. This is similar to popping a clutch on a manual transmission car. The hoist would bog down, and the workers would mechanically hold the hoisting line while the hoist built up power again. Then, the hoist would be re-engaged “shocking” and possibly damaging the cable as it strained to lift it.
Recommendation #2: Employers should ensure that adequate rescue equipment/personnel are available.
Discussion: There was no site-specific accident prevention plan available for this job. The company trains their personnel on basic tower rescue techniques during orientation. These are effective under “assumed” emergency conditions. In this case, the position of the victim made rescue impossible by company personnel. The owner stated that he does not contact local emergency personnel services in the areas they work prior to starting a job. The local fire chief stated that they did not have anyone qualified to climb the towers, but they are planning on putting together a “tower rescue” plan in the future. It is recommended that rescue personnel be notified when work ion this type of tower is anticipated to determine where nearest tower rescue team is located and the procedures necessary to ensure their availability.
Recommendation #3: Employers should routinely conduct scheduled and unscheduled worksite safety inspections.
Discussion: Equipment that was either damaged or used improperly prior to this incident may have contributed to this fatality. Regular site visits by company owners and general contractors help to identify unsafe work practices and trend areas. These visits should be documented with the problem area noted, recommended corrective actions, and the person responsible for ensuring the corrections are completed.
Recommendation #4: Employers should supplement worker training on safe work practices with discussions of FACE case reports and other related training aids.
Discussion: There are currently an estimated 200,000 communications towers across the United States, including about 275 broadcasting towers that are 1,500 feet or higher. Every day new towers are being erected. According to NIOSH, since 1992 there have been 163 employees killed in communications tower incidents. In the 18 months previous to this incident at least 14 people have died nationally involving communications towers. There are many sources of training materials available, including FACE case report, trade magazines, etc. Learning from others mistakes is certainly acceptable as a means of improving a company’s overall safety program.
Recommendation #5: Tower owners should, through the use of contractual language, ensure that employers/workers adhere to OSHA-required safety measures (including Compliance Directive 2-1.29) while construction or maintenance is being performed on their towers.
Discussion: Involvement by all parties (tower owners, engineers, contractors, safety personnel, etc.) in the drafting, awarding and safe completion of any erection, maintenance or modification contract for telecommunication towers is necessary to ensure the identification and/or elimination of all known safety concerns. General safety clauses may be inserted into the contract which call for the “contractor” to abide by all Federal, State, County and local safety guidelines. All or part of these may be specified in the contract, to include, but not limited to site specific safety & health programs, fall protection issues, equipment inspection procedures, emergency response methods, etc.
REFERENCES: (top)
-
OSHA Part 1926 Code of Federal Regulations for Construction Standards.
-
OSHA park 1910 Code of Federal Regulations for General Industry.
-
OSHA Instruction Directive Number: CPL 2-1.29
-
NIOSH Alert Publication No. 2001-156, Preventing Injuries and Deaths from Falls during Construction
and Maintenance of Telecommunication Towers
-
NIOSH Publication NO. 2000-116, Worker Deaths by Falls – A summary of Surveillance Findings and
Investigative Case Reports
ATTACHMENTS: (top)
|
|
|
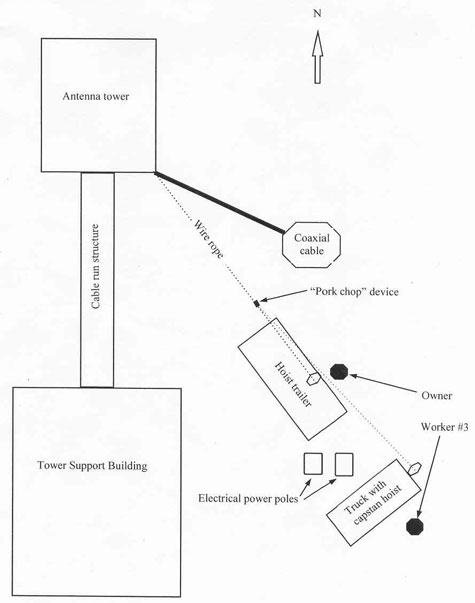
Site diagram. Approximate positioning of equipment and
personnel at the time of the accident.
|
|
|
|
Picture #1 - View of telecommunications tower.
|
|
|
|
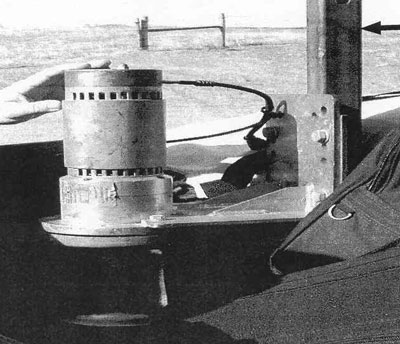
Picture #2 - Control box on hoist trailer.
|
|
|
|
Picture #3 - Hoist trailer.
|
|
|
|
Picture #4 - Separated wire rope.
|
|
|
|
Picture #5 - Coaxial cable section.
|
|
|
|
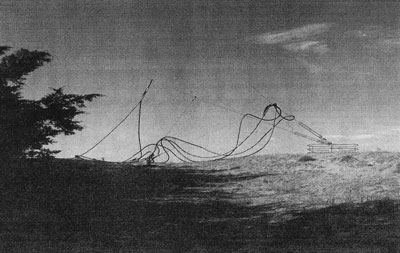
Picture #6. Coaxial cable and wire rope laying over guy wires.
|
|
|
|
Picture #7. Electrical capstan’s hoist.
|
To contact Nebraska State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
|